
Overview
1. Quick Crash Course in Hamstring Anatomy
2. Differentiating Strains and Tendinopathies
3. Rehab Direction
4. Getting Back to Classes and Rehearsals
Hey dancers! If you’ve been silently suffering from pain in the back of your thigh (close to your sit bones) that comes on after doing kicks or deep stretches, you might have a high hamstring injury.
Some common complaints I hear are:
- Pain at the back of the thigh (below buttocks) when getting into front splits
- Pain in forward folds during warm up
- Feeling slightly better after stretching, but nagging soreness and/or pain comes back after class
- Feeling restricted in kicks
To properly rehab the hamstrings and get stage ready, we need to know 2 things:
- Which area of the hamstrings are injured, and what the original movement was?
– This tells us what we need to work on in later stages of rehab to prevent re-injury when performing similar movements - Is it a strain or tendinopathy?
– This guides our rehab direction
1. Quick Crash Course in Hamstring Anatomy
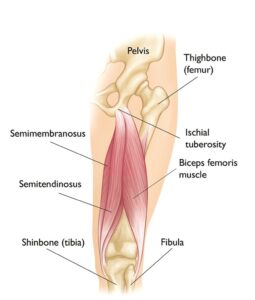
Primary movement: knee flexion (bending the knee)
Secondary movement: hip extension
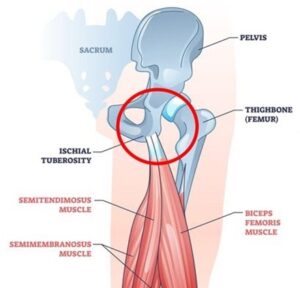
Muscle origin: ischial tuberosity (aka our sit bones)
Muscle insertion:
- Medial tibial condyle (semimembranosus, semitendinosus)
- Fibular head, lateral tibial condyle, and posterior aspect of the lateral intermuscular septum (biceps femoris)
2. Differentiating Strains and Tendinopathies
Strain: damage to muscle fibers caused by a high amount of mechanical stress on the hamstrings, either through excessive loading, or sudden extension/stretch
- In dancers: commonly occurs during front splits training (hamstring length), or penche kicks (strength in a lengthened position)
Tendinopathy: pain and dysfunction in a tendon, that is associated with a specific movement or activity
- Tendon is a tissue that connects muscle to bone
- Serves several purposes: absorbing tensile forces (parallel to the muscle), acting as a spring, and changing the direction of pull on a muscle by encasing a bone pulley (e.g. kneecap)
- Normal tendon response to load: stiffen and adapt to the demand placed on it if given an appropriate amount of load and sufficient recovery time
Strain | Tendinopathy | |
Mechanism of injury | High mechanical stress on muscle fibres – excessive loading or stretching | Overloading and/or insufficient recovery time à disrepair from failed healing response |
Signs and symptoms | ·Pain over injury site, pain on palpation ·Possible bruising depending on severity ·Weakness and pain with hamstring muscle contraction ·Possible pain with walking | ·Nagging ache in buttocks when sitting or stretching ·Hamstring tightness or soreness after sitting for a while ·Delayed soreness in glutes or back of knee after dance class or rehearsal |
Classification | Grade I: mild tear, < 5% Grade II: partial tear, ~50% Grade III: complete rupture | High hamstring tendinopathy (proximal): inflammation and degeneration of hamstring tendons attaching to ischial tuberosity
Low hamstring tendinopathy (distal): inflammation and degeneration of hamstring tendons attaching to shin bones |
Common symptoms in dancers | ·Temporary relief (5-10 min) with stretching ·Sharp pain with sudden hamstring contraction or lengthening ·Feeling weaker with hamstring contraction | ·Pain or soreness during warm ups that goes away during class, but returns after cool down ·Deep ache close to the buttocks |
Common dance movements provoking pain | ·Front kicks ·Front splits ·Standing forward fold | ·Deep squats in parallel ·Deep lunge ·Tabletop position |
3. Rehab Direction
Strain
- Muscle healing (isometrics, reduce pain and inflammation)
- Strengthening: heavy and slow concentrics in controlled ranges
- E.g. hamstring bridging

- Late stage strength: eccentric strength, adding power, speed, plyometrics
- E.g. Romanian deadlifts for eccentric strength, bridge with jumps for plyometrics

For dancers’ rehab: ensure progressive build up to the movement(s) causing the initial injury
Aim for strength even in end-range movements e.g.
Late-end stage rehab should start incorporating dance-specific movements to provide sufficient challenge and loading for the hamstrings
Tendinopathy
- Promote tendon healing – isometrics, eccentric strengthening
- Progressive overload and re-introducing plyometrics for tendon elasticity
For dancers’ rehab:
Ensure sufficient tendon healing before introducing tendon elasticity training
Gradual transition from advanced strength exercises to dance-specific movements – important not to overload or underloading
4. Getting Back to Classes and Rehearsals
Consider common movements in your main dance genre and break them down to pre-requisites i.e. does the move require more hamstring length or strength?
One way of approaching it is to assess what is lacking, e.g. if you can do a hamstring stretch but have difficulty holding your penche, most likely you need to work more on hamstring strength in a lengthened position. Versus if you have great range in your Romanian deadlift but you just can’t reach a flat grand jete, you might need to work on hamstring length in front splits.
Some movement examples are:
– Contemporary dance
- Tabletop warm ups (strength in a lengthened position)

- Illusion kicks (supporting leg – strength in a lengthened position)
– Ballet
- Arabesque penche (supporting leg – strength in a lengthened position)
- Grand jete (front leg – length during high point of jete, eccentric strength when landing)
– Jazz
- High kicks (working leg – length to kick, strength for fast descent)

- Penche kicks (supporting leg – strength in a lengthened position)
– Hip hop
- Quick weight shifts, pivots (working leg – quick deceleration)
Other points to consider for training:
- Incorporating endurance training to ensure sufficient muscular endurance for a full-length class or rehearsal
- Strengthening muscle groups around the hip and knee e.g. glutes, quads, calves
- Working on strength as a supporting leg vs as a working leg