
90% of injuries in dancers involve the low back, pelvis, legs, knees, or feet (Koutedakis and Jamuris, 2004). Prolonged bouts of training with inadequate rest, unsuitable floors, difficult choreography, and insufficient warm-ups are among the factors that contribute to dance injuries.
One of the most common knee injuries in dancers is patellofemoral pain syndrome (PFPS).
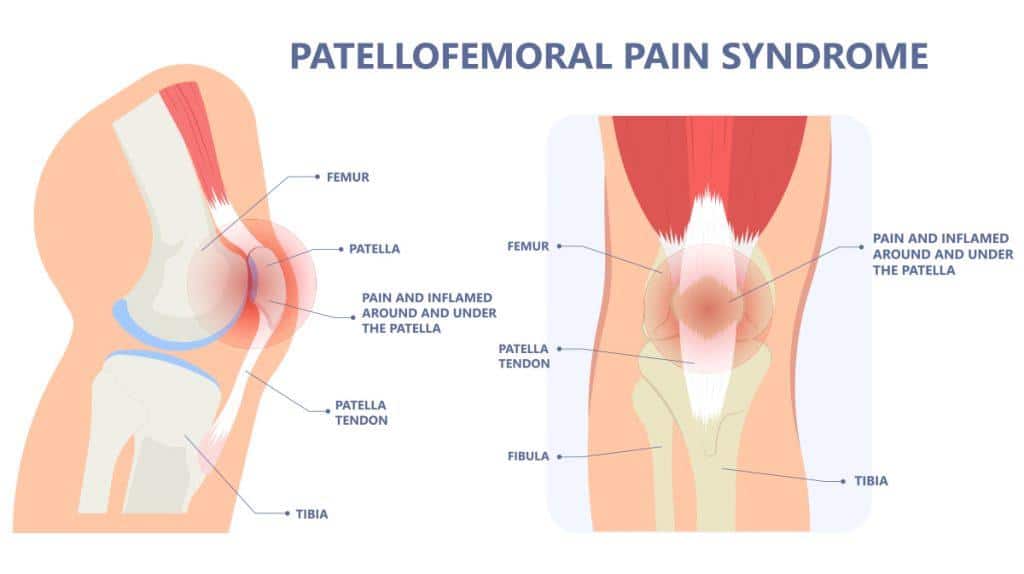
What is Patellofemoral Pain Syndrome (PFPS)?
It is a general term for pain around, or behind the knee cap. This condition is more common in women than men, and most often affects younger individuals between 10 to 35 years old.
Common symptoms
· Pain with ascending and/or descending stairs
· Pain with squatting
· Pain after prolonged sitting
· Grinding sensation in the knee
· Clicking or cracking that is accompanied with pain
Contributing factors
· Sudden overload
o Sudden increase in training intensity, frequency, or volume
· Kneecap misalignment or poor tracking
· Muscle imbalance in quadriceps or glutes
· Muscle tightness in iliotibial band, quadriceps, hamstrings
· Knee hyperextension
· Dance-related movements
o Eccentric loading and repeated landing e.g. plié, jump landing
o Forced turnout with knee or ankle compensation
o Limited ankle mobility affecting plié depth
o Dancing on hard surfaces
o Dancing in heels
How can physiotherapy help with PFPS?
We will perform a thorough assessment to identify the factors contributing to your symptoms. This helps us to tailor your treatment accordingly.
Hands-on techniques may include soft tissue release, knee cap mobilisations, dry needling in order to increase mobility or reduce tightness in relevant muscles.
Individualized exercise programs will be given to target the factors identified during the assessment e.g. strength deficit, mobility restrictions.
Timeline for recovery depends on how long you have had symptoms prior to seeking treatment. Generally, dancers with newer symptoms can recover in 4-6 weeks. Someone who has been having pain for a while may take close to 3 months to see improvements. Hence it is very important to seek treatment as soon as possible instead of adopting the “wait and see method”.
Do I have to stop dancing completely?
Being injured does not automatically mean you have to stop training. Unless absolutely necessary, we prefer not to stop training completely. We will work together to modify your routines so that you can still continue training and working on choreography without aggravating your pain. E.g. if you have a knee injury, you can still work on upper body or hip strength and flexibility. This also helps to prevent deconditioning during the recovery process, and less of a gap to return to where you were pre-injury.
I’m already dancing so much, do I still need strength training? Will strength training make me look bulky?
Proper hip strength and neuromuscular control (especially in hip abductors and hip external rotators) enhances knee stability by controlling the pelvis, and limiting hip adduction and internal rotation that contributes to increased knee valgus during dance movements. Targeted strength training as part of a rehab program will address the areas of weakness contributing to your knee pain, and also helps make you a stronger dancer overall.
Strength training is closely related to neural adaptations which increase muscle strength. These neural mechanisms include alterations in agonist-antagonist co-activation, increases in motor unit firing rates, and changes in descending drive to the motor neurons.
There is strong evidence that strength training decreases incidence of dance injuries, without interfering with artistic or aesthetic requirements of a dancer (refer to our previous posts on strength training for dancers). Increases in muscle strength are not necessarily accompanied by proportional changes in muscle size (MacDougal et al).
What are some common rehab exercises for PFPS rehab?
Exercises targeting
· Hip external rotators e.g. clamshells
· Hip abductors e.g. sidelying leg lifts
· Core stability
· Quadriceps strength
Proprioceptive training
Even with unilateral PFPS, proprioception is decreased in both knees. Pain-free proprioceptive exercises will be included in the rehab program, especially when preparing dancers to return to full intensity of training.
Are there any other possible reasons for my knee pain?
Other possible diagnoses include, but are not limited to: patella tendinopathy, ligament sprain, meniscus injury, ITB friction syndrome. Knee pain can also be a presenting symptom (referred pain) when the cause is at a different joint e.g. hip or ankle.
The knee joint is made up of many structures that can contribute to pain or inflammation, hence a detailed assessment is required before we can provide a definite diagnosis.
If you think you might have dance-related PFPS and you’d like a session to get it checked out, reach out to us via WhatsApp (8023 3805) or our Instagram page (@activexphysio).
References
Koutedakis Y, Jamuris A. The dancer as a performing athlete: physiological considerations. Sports Med. 2004;34:651–661.
MacDougall J, Elder G, Sale D. Effects of strength training and immoblization on human muscle fibers. Eur J Appl Physiol Occup Physiol. 1980;43:25–34.
Sohl P, Bowling A. Injuries to dancers: prevelance, treatment, and prevention. Sports Med. 1990;9:317–322.
Welsh, C., Hanney, W. J., Podschun, L., & Kolber, M. J. (2010). Rehabilitation of a female dancer with patellofemoral pain syndrome: applying concepts of regional interdependence in practice. North American journal of sports physical therapy : NAJSPT, 5(2), 85–97.