

Mobility Training for Injury Prevention & Recovery to Runners - What Actually Matters
A recap of my talk at the Standard Chartered Lunch Time Running Clinic 2025.
What is mobility?
Mobility = usable Range of Motion (ROM) under control that supports the loads of running. Passive flexibility without control does not transfer to better mechanics or lower risk. Do note mobility work is the support act; strength and load management do the heavy lifting for injury risk reduction (Lauersen, Andersen and Andersen, 2018).
Why mobility matters in running
Ankle dorsiflexion
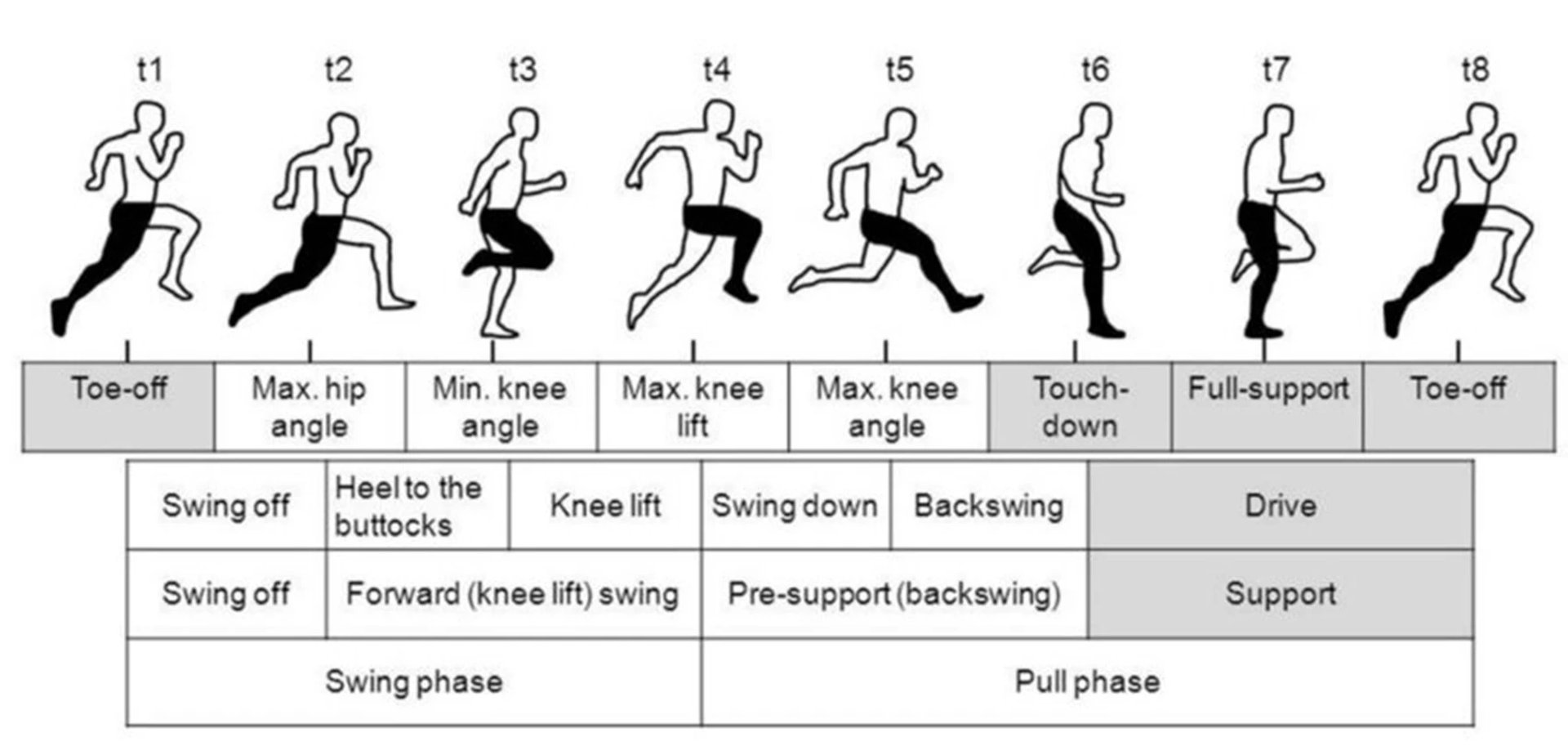
From touchdown through to full support/mid stance phase, adequate dorsiflexion range is needed to allow the tibia (shin bone) to move forward over the foot, without upstream compensations. Restricted dorsiflexion is linked to stiffer landing mechanics, more frontal‑plane knee motion, and higher patella-femoral loads, all of which can increase the risk of injury.
Hip extension
During the toe‑off phase of running, the hip moves into approximately 10 degrees of hip extension. Without adequate range here, there will be increased anterior pelvic tilt and/or lumbar extension in order for the body to ‘gain’ the range, potentially leading to low back pain. The limited mobility could come from hip flexor tightness or a stiff hip joint into extension.
Thoracic rotation and arm swing
Efficient running needs controlled thoracic rotation that couples with arm swing to counter leg‑generated angular momentum. Adequate thoracic mobility lets this counter‑rotation happen without borrowing from the lumbar spine.
What actually lowers injury risk?
Strength training
Across multiple randomised trials and sports, strength training shows the largest and most consistent prevention effect. Stretching alone does not.
Load management
Risk spikes when a single run leaps beyond your recent capacity. New 2025 cohort data (approximately 5,200 runners) show injury rates climb when any one run exceeds around 10% of your longest run in the past 30 days; much bigger jumps raise risk sharply. Older data in novice runners echo the same direction where greater than 30% progressions in short windows carry more injuries (Frandsen et al., 2025). As a rule of thumb, no more than 10% increase to total running volume per week.
The “forgotten” muscle: The soleus
During stance phase to toe off, the calves, especially the soleus are major contributors to support and propulsion. Studies show the Achilles tendon can see roughly 6–10× body weight during running/sprinting, and calf muscle-tendon unit forces can approach around 12× body weight at higher speeds. The soleus dominates vertical support across speeds and since it’s also predominantly slow‑twitch, it’s highly utilised in running. This muscle needs to be strengthened to prevent knee, ankle and calf injuries (Adam et al., 2023).
How to train it?
- Bent‑knee calf raises (seated or standing) to bias soleus: 3–5 sets of 8–12 repetitions (reps) heavy, controlled 2–3 days/week; progress load.
- Pair with straight‑knee calf raises to load gastrocnemius so the whole calf complex. Incorporate it in your strength program twice a week.
How to ‘gain’ mobility? What the evidence supports.
Static stretching (long holds)
- Pre‑run: Long holds (≥60 seconds per muscle) acutely reduce strength and power. Keep static holds brief if used at all before running however we recommend best to use it post-run.
- Post‑run: Static stretching increases ROM. Current dose‑response meta‑analysis suggests little extra benefit beyond 4 minutes per session or 10 minutes per week per muscle group (Ingram et al., 2024).
- Practical Guidelines: 2–3 sets of 30–60 seconds for key areas, 5–10 minutes/week per muscle group post run or outside your runs.
Dynamic stretching
- Pre-run: Best used for the warm‑up as it raises temperature, increases joint angles needed for running and improves readiness without negatively affecting performance.
- Practical Guidelines: 8–12 reps or 30–60 seconds per drill pre-run.
Foam rolling (self myofascial release)
- Acute range of motion gains and small‑to‑moderate reductions in Delayed Onset Muscle Soreness (DOMS) without harming performance.
- Practical Guidelines: Effective bouts cluster around 60-120 seconds per muscle pre or post run to reduce DOMS and sensation of ‘tightness’.
Read further on how to maintain long lasting mobility changes here: https://activexphysio.com/guide-to-creating-lasting-mobility-changes/
A simple runner’s mobility routine
Pre run (7–10 minutes, dynamic)
- Calf raises on a step (smooth tempo through full range): 2×12–15.
- Runner’s lunge with thoracic spine (T‑spine) rotation: 6–8 rotations/side.
- Leg swings (front‑to‑back and side‑to‑side): 15–20/leg each plane.
- Walking quadriceps stretch (grasp ankle, slight hip extension, opposite arm reach): 10–12/side.
- “Roll the carpet” hamstring scoops: 10–12/leg.
- Optional 30–60 seconds foam rolling calves and quads if you feel stiff
Post run (8–10 minutes, static + rolling)
- Calf stretch (knee straight) then soleus stretch (knee bent): 2–3×30–45s each.
- Half‑kneeling hip‑flexor & quadriceps stretch: 2–3×30–45s/side.
- Hamstring stretch: 2–3×30–45s/side.
- Tensor Fasciae Latae (TFL) side stretch: 2×30–45s/side.
- Foam roll calves, quads, glutes, hamstrings: ~60–120s/muscle.
Bottom line for race prep
- Build and keep the ankle, hip, and thoracic ROM you can control.
- Prioritize strength especially the soleus and the big hip/knee extensors.
- Avoid single‑run distance spikes; keep long‑run progressions conservative and no more than 10% increase per week.
- Use dynamic mobility before the run, static plus foam rolling after the run.
References:
- Lauersen, J.B., Andersen, T.E. and Andersen, L.B. (2018) Strength training as superior, dose‑dependent and safe prevention of acute and overuse sports injuries: a systematic review, qualitative analysis and meta‑analysis. British Journal of Sports Medicine, 52(24), pages 1557–1563. Digital Object Identifier (DOI): 10.1136/bjsports-2018-099078.
- Novacheck, T.F. (1998) ‘The biomechanics of running’, Gait & Posture, 7(1), pages 77–95.
- Frandsen, J.S.B., Hulme, A., Parner, E.T., Møller, M., Lindman, I., Abrahamson, J., Simonsen, N.S., Jacobsen, J.S., Ramskov, D., Skejø, S., Malisoux, L., Bertelsen, M.L. and Nielsen, R.O. (2025) ‘How much running is too much? Identifying high-risk running sessions in a 5200-person cohort study’, British Journal of Sports Medicine.
- Adam, N.C., Smith, C.R., Herzog, W., Amis, A.A., Arampatzis, A. and Taylor, W.R. (2023) ‘In vivo strain patterns in the Achilles tendon during dynamic activities: a comprehensive survey of the literature’, Sports Medicine, 53(9), pages 1819–1839.
- Ingram, L.A., Tomkinson, G.R., d’Unienville, N.M.A., Gower, B., Gleadhill, S., Boyle, T. and Bennett, H. (2024) ‘Optimising the dose of static stretching to improve flexibility: a systematic review, meta-analysis and multivariate meta-regression’, Sports Medicine, 54(2), pages 251–270.



